Abstract
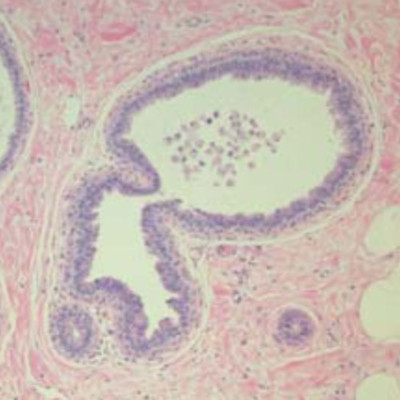
Columnar cell lesions (CCLs) are one of the most common abnormalities in the adult female human breast, characterized by the presence of columnar-shaped epithelial cells lining enlarged terminal-duct lobular units. CCLs are being seen increasingly in core biopsies taken for the non-palpable calcifications. The increased incidence may reflect improved delineation and recognition of CCLs by pathologists or a true increase in incidence related to biological and/or environmental factors. Columnar cell-like lesions have been described under a variety of names such as blunt duct adenosis, flat epithelial atypia, and ductal intraepithelial neoplasia type DIN1a. The current histologic classification used by some pathologists divides them into simple columnar cell change and columnar cell hyperplasia, both of which can occur with or without atypia. Columnar cells lack mature luminal or basal/myoepithelial phenotype markers, but they are usually positive for estrogen receptor-alpha. The cellular origin of CCLs and their possible relationship to either expansion or metaplasia of a preexisting normal cell phenotype remains unclear. CCLs are frequently associated with lobular and ductal in situ tumors and invasive lobular and tubular carcinomas. The relationship and natural history of CCLs to invasive ductal carcinoma is enigmatic, but they may prove of clinical relevance when detected by screening mammography.